About this report
This report is aimed at anyone interested in people’s health and wellbeing across mid and south Essex and beyond. It highlights how partners across multiple sectors are collaborating and engaging with local populations to really understand people’s experiences and what they need.
If you would like to download a fully designed version of this report please click the link below.
Introduction
People’s life chances are largely determined by where they are born and the circumstances they’re born into. In mid and south Essex, people in some neighbourhoods die 13 years earlier than others living less than a mile away and spend many more years living in poor health, through no fault of their own.
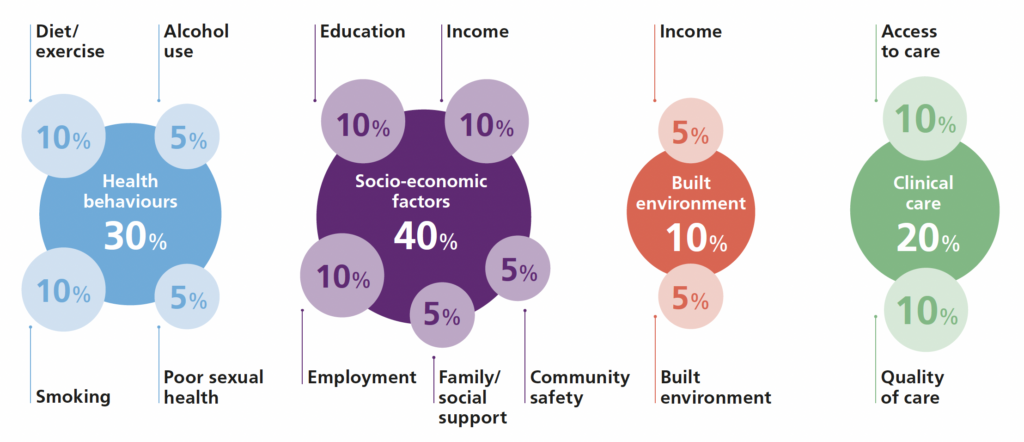
These health inequalities are caused by a combination of the economic, environmental and social circumstances people live in (the wider determinants of health). These factors are responsible for 80 per cent of our health outcomes. And they are preventable. By taking action across the system, we can do something about it.
This report highlights our work across Mid and South Essex Integrated Care System (MSE ICS) to tackle health inequalities. It shows what is possible, even in today’s harsh economic climate, when we take a collective approach to narrowing the gap. We hope it will inspire you to find ways to tackle health inequalities through your work.

This report demonstrates how Mid and South Essex Integrated Care Partnership has been taking action to deliver on our common endeavor to reduce health inequalities. We are working together to understand the avoidable health and care inequalities facing our communities and partnering with them to build healthier and more resilient communities. We hope everyone who reads this will join us in working to narrow the gap
80% of health inequalities are caused by a combination of the economic, environmental and social circumstances people live in.
What do health inequalities look like?
Public health bodies have flagged health inequalities for many years. But the Covid-19 pandemic had an unequal impact on different population groups and widened existing health inequalities.
The pandemic also brought local organisations and individuals together to find innovative solutions to shared problems. When MSE ICS was created, it sought to build on this learning. Its aim is to bring local players together to develop new ways of working across neighbourhoods, local areas and different parts of the system.
Only 20% of our health is affected by health services. The remaining 80% is caused by the wider determinants of health.
What are health inequalities?
NHS England describes health inequalities as: “the unfair and avoidable differences in people’s health across the population and between specific population groups. They do not occur randomly or by chance. They are socially determined by circumstances largely beyond an individual’s control.”
Health inequalities occur as a consequence of a number of factors, such as socioeconomic disadvantage, including employment opportunities, housing and employment. This means that reducing inequalities is a complex undertaking. No single action or organisation can reduce inequalities alone: the work requires a sustained, organised, collaborative focus.
Healthcare inequalities also refers to inequity in the way healthcare services are provided. This can affect people’s opportunity to access care or to lead healthy lives. For example, people from disadvantaged areas are often under served by healthcare services and, as a result, to experience poorer health outcomes. This is called the ‘inverse care law’.
What factors drive good health outcomes?
Health inequalities in mid and south Essex
- An estimated 133,000 people (10.7% of the whole MSE population) live in the 20% most deprived areas nationally
- More than 6 in 10 adults in MSE are either overweight or obese
- Gap in life expectancy in some areas as much as 10 years between our wealthiest and most deprived neighbourhoods
- Smoking prevalence in adults in MSE is 14.2% compared to England average of 12.7%
- Life expectancy variations:
- 82.4 years for females living in Thurrock
- 84.7 years for females living in Brenwtood
- 78.3 years for males living in Thurrock
- 81.3 years for males living in Chelmsford
- Top three contributors to premature mortality attributable to social-economic inequality
- cancer
- cardiovascular disease
- respiratory disease
- Top 3 risk factors with greatest impact on population health and health inequalitities:
- tobacco
- blood pressure
- dietary risks
Health inequalities are not inevitable and can be significantly reduced.
Professor Sir Michael Marmot
How the work fits together
Tackling health inequalities across a geographical region such as mid and south Essex is not a linear process. Change happens through a complex web of activities sparked by connections, collaboration, and the exchange of resources and data.
These partners operate at three main levels, each of which contributes unique strengths.
Balancing need
Tailoring the priorities of the system and the alliances to the specific needs of each neighbourhood requires some flexibility. But all the actions we all take, as partners, complement one another’s efforts and work towards our common goal of reducing health inequalities.
Mid and South Essex Integrated Care System
- 149+ GP practices operating from over 200 sites
- 3 main community and mental health service providers
- 1 ambulance Trust
- 3 Healthwatch organisations
- 9 voluntary and community sector organisations
Basildon and Brentwood
- Population of 285,000
- 6 Primary care networks
- 5 in Basildon
- 1 in Brentwood
Mid Essex
- Population of 405,000
- 9 Primary care networks
- 3 in Chelmsford
- 2 in Braintree
- 3 in Maldon/Chelmsford
- 1 in Maldon/Braintree
- 1 in Braintree/Chelmsford
South East Essex
- Population of 377,000
- 8 Primary care networks
- 2 in Castle Point
- 2 in Rochford
- 4 in Southend
Thurrock
- Population of 176,000
- 4 Primary care networks
- 1 in Tilbury and Chadwell
- 1 in Grays
- 1 in Purfleet
- 1 in Corringham
Who’s who?
Health inequalities partners in mid and south Essex
Where I work, as a GP, some of our patients are heavily weighed down by the lack of money to put food on the table or top up their electricity meter. If we look at their issues simply through a ‘health’ lens we are missing the more fundamental problem: people’s socioeconomic status and other wider determinants.
Dr Anita Pereira, GP and Chair, Essex Faculty, RCGP, MSE ICB | Clinical Lead, Health Inequalities and Personalised Care
When the system came into being, I was very excited. Increasingly, GPs are working alongside community and mental health services, the voluntary sector and others, sharing expertise in trauma-informed care, bridging cultural and language barriers and putting in place innovative solutions.
Our job is to understand how health inequalities play out differently in each neighbourhood, with its unique characteristics, personality and flavour. We chart the community assets and use our local insights to enhance provision and inform our strategy.
Anthony Quinn Chief Executive,
Our Alliance Partnership brings together voluntary sector organisations alongside other agencies such as police and fire services. Health inequalities must run through all our work if we are to tackle the wide breadth of factors that lead to health inequalities.
Southend Council for Voluntary Services | Chair, Southeast Alliance
For a long time, health inequalities and the wider determinants of health were mostly the preserve of public health. Now these issues are being discussed and embraced by partners across the system. There’s still work to be done, but I feel enthused and quietly optimistic.
Krishna Ramkhelawon Director of Public Health, Southend-on-Sea City Council
We’ve spent the past year helping the ICB develop its ten-year strategy and combining our population health improvement programme and health and wellbeing priorities. I’m really pleased that we are prioritising babies, children and young people. Investing in early support improves wellbeing and outcomes throughout our lifespan, from dental health and obesity to education and employment.
Our approach
In MSE ICS, our work to address inequalities is guided by our ambition to improve population health outcomes. We are doing this by understanding and then addressing the drivers of those inequalities.
The figure below shows our population health framework (adapted from The King’s Fund framework), which enables us to focus on delivering integrated care. This goes further than treating ill health: moving towards a proactive, preventative model of care to address the causes of poor health outcomes and the wider socio-economic determinants of health.
The figure shows the four key pillars of the framework (in the four coloured segments) and the enablers that are needed to make it happen (in the purple circles).
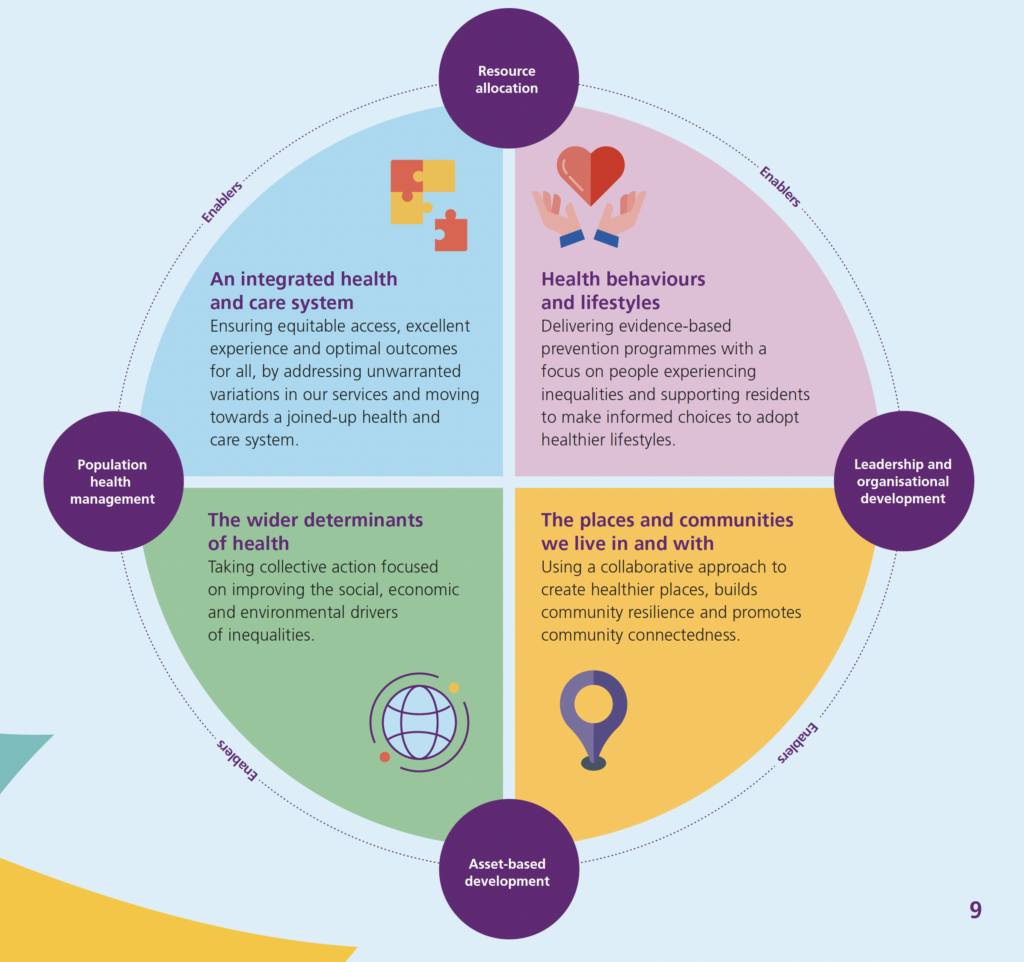
The mid and south Essex population framework
The image is a circular diagram divided into four quadrants, each describing a key focus area for resource allocation. The diagram also highlights overarching themes such as “Population health management,” “Enablers,” “Leadership and organisational development,” and “Asset-based development.” Here’s a plain text description of the content:
An integrated health and care system (top-left quadrant, light blue)
Focus: Ensuring equitable access, excellent experience, and optimal outcomes for all.
Goal: Addressing unwarranted variations in services and moving towards a joined-up health and care system.
Health behaviours and lifestyles (top-right quadrant, light pink)
Focus: Delivering evidence-based prevention programmes.
Goal: Concentrating on people experiencing inequalities and supporting residents to make informed choices to adopt healthier lifestyles.
The wider determinants of health (bottom-left quadrant, light green)
Focus: Taking collective action to improve social, economic, and environmental drivers of inequalities.
Goal: Addressing the broader factors that influence health outcomes.
The places and communities we live in and with (bottom-right quadrant, light yellow)
Focus: Using a collaborative approach to create healthier places.
Goal: Building community resilience and promoting community connectedness.
Central Themes:
Resource allocation (centre-top, purple circle)
Population health management (left, purple circle)
Enablers (top and right, purple circles)
Leadership and organisational development (right, purple circle)
Asset-based development (bottom, purple circle)
Each quadrant is connected to these central themes, illustrating how these focus areas are interrelated and support the overall goal of improving health outcomes and equity.
The four enablers shown in Figure 2 focus on the following areas of work:
Resource allocation. Developing sustainable funding strategies to address inequalities, allowing investment in transformation at a scale and intensity proportionate to the level of disadvantage.
Population health management. Helping front line services understand current health and care needs and predicting what local people will need for the future.
Leadership and organisational development. Developing human learning systems that foster a culture of shared learning and innovation, supported by infrastructure to build capacity and leadership.
Asset-based development. Working closely alongside communities, using an asset and strength-based approach to develop local solutions and build resilience.
Our framework helps us ensure that each health inequalities activity, across the system, is:
- focused on a health gain for a defined group that contributes to a shared outcome in the MSE outcomes framework
- using appropriate evidence to identify the group in need, including integrated data, analytics and intelligence
- drawing on insight, resource and commitment to design appropriate interventions.
What we’re doing
Our vision is of a health and care partnership working for a better quality of life in a thriving mid and south Essex, with every resident making informed choices in a strengthened health and care system.
Addressing health inequalities plays a key role in that ambition. Over the coming pages each of these themes is explained, with examples of specific projects taking place in this area:
- Theme one: Integrated health and care system
- Theme two: Our health behaviours
- Theme three: The places and communities we live in and with
- Theme four: Wider determinants of health
Theme one: Integrated Health
As the new health and care structures evolve, the barriers between organisations and sectors are coming down. Multi-disciplinary teams are working in a more integrated way, with people stepping outside of their silos to support each other for the benefit of the individuals they support.
Gradually, the system is working in a much more integrated fashion.
But this is only the start of the journey. Integration requires people to pool knowledge, skills and resources. Ultimately, this will save resources. Most importantly, it enables care to put the individual at the centre – an essential ingredient in tackling health inequalities.
Comprehensive assessment and treatment for multiple diseases
Primary care network staff, including GPs, practice nurses, health coaches and social prescriber link workers, are delivering multi-morbidity clinics across Thurrock Alliance.
The integrated service offers diagnosis and management of hypertension, cholesterol and depression and offers support with smoking and weight loss.
The clinics are delivered alongside local authority lifestyle services and specialist mental health practitioners. The model is being rolled out across MSE.
A holistic approach
Benfleet Primary Care Network is taking a holistic approach to residents’ wellbeing to prevent more severe conditions in the future. The initiative is focusing on 63 residents aged 60–74 with multiple complex health issues such as depression, hypertension and diabetes.
The team supports residents to explore their personal goals, financial constraints and social support networks and then direct them to support such as weight-loss classes or therapy.
Integrated discharge
The Integrated Discharge Pathway, co-funded by MSE ICS and NHS Foundation Trust, supports patients – particularly those who are older or frail – to transition smoothly from hospital to home.
By addressing complex needs, it ensures a seamless discharge into the community, getting people home sooner, with shorter hospital stays, faster recovery times, reduced risk of readmission and faster recovery.
Theme two: Healthy Behaviours
Supporting people to adopt healthy behaviours focuses on investing in people’s health, through prevention strategies. These range from pregnancy support – giving children the best start in life –
to helping adults stop smoking or manage their weight.
Traditionally, if someone was overweight they might be referred to a 12-week weight-loss programme. But if they can’t travel beyond their corner shop to buy fresh fruit and vegetables, long-term improvement is unlikely.
By working as a whole system, we can work to create environments that support healthy living by changing the food landscape and improving green spaces. We can also make sure all services take a ‘making every contact count’ approach – with professionals gently mentioning smoking or healthy diet every time they meet someone.
Eventually, this can help people start to make very small changes.
Pedal power
Essex Pedal Power provides free bikes to encourage residents in disadvantaged communities to become more active. It also improves access to employment, training, educational opportunities and local services.
The project, run by Active Essex with Essex County Council and others, includes cycle and bike maintenance training. By January 2024 more than 1,000 people had received bikes, cycling 224,987km.
Smoking cessation
A stay in hospital can be hard to manage for someone with a smoking habit. The acute trust is now offering patients staying overnight behavioural support, nicotine replacement therapy or other pharmacotherapy during their stay. After they return home they receive follow up and referral to
community services.
The maternity service is also delivering a programme to reduce smoking during pregnancy.
Child oral health
MSE has agreed a systems approach to help improve children’s oral health. In 2022/23
we committed health inequalities funds to implement supervised toothbrushing schemes in two of our four alliances.
We have also been running a pilot to implement evidence-based interventions alongside universal early years services. Results are showing increased access to dental care for children.
Theme three: Communities
An important element of our work to tackle health inequalities involves taking a place-based approach.
That means taking the time to understand our communities – not just the challenges they face, but also the assets they have, such as community activities and social networks. These differ from one community to the next, depending on who lives there and a host of other circumstances.
Only once we understand their needs can we help them address the challenges they face, drawing on their assets to build community resilience. This can help people manage daily life and be better prepared for shocks such as the Covid-19 pandemic or the cost-of-living crisis.
The role for formal structures within the system, such as healthcare providers and local authority teams, is to understand all of those assets within our communities and work collectively with them. This helps us become more connected to the people we serve.
Fella’s Fair
Fella’s Fair runs events to promote awareness of support charities, men’s physical health and wellbeing, networking sessions and guest speakers with refreshments. The events are held at football stadiums during their match day. They are delivered by the charity Healthwatch Essex working in collaboration with sports associations, sports clubs in Essex, men’s health charities and current networks.
Health and wellbeing café
West Basildon PCN and the charity Achieve, Thrive Flourish have established a wellbeing café and meeting venue. Supported by several statutory and community organisations, it hosts activities including social clubs, exercise groups, a crèche, arts and crafts activities and health-related talks.
The centre has an open-door policy for local residents with specific invitations to people from the most deprived areas and disadvantaged groups.
Community Connectors
A group of community volunteers either living with, or caring for someone with, chronic obstructive pulmonary disease (COPD) are sharing their lived experience to shape future services. Their work has led to a COPD drop-in, now running weekly due to demand.
They have also worked with the pulmonary rehabilitation team to design a ‘stretch and breathe’ class, with 19 sessions attended by around ten people per class.
Theme four: Wider determinants
Our system’s work on the wider determinants of health operates at two levels: supporting with day-to-day issues and developing the local infrastructure for more sustainable change.
Individual support is delivered by community and voluntary sector organisations. In healthcare, social prescribers and care coordinators are supporting people with the wider factors that affect their health.
So if someone’s health is affected by housing or loneliness, a social prescriber may contact the housing team for them or link the person into a local support group. This moves the boundaries beyond medical concerns to a focus on the whole person.
Sustainable improvement involves analysing system-wide data. If we spot a higher incidence of a condition in certain communities, then we can identify the causes – say, lack of employment opportunities, isolation or poor health literacy – and then work with partners to develop a long-term plan.
Health inequalities microgrant-funded project
In 2022 MSE ICS offered microgrants of £500–£1500 to support projects and initiatives addressing health inequalities locally. More than 1,689 people have accessed support across more than 60 projects, with 148 people receiving support from ethnic minority-led recipient organisations.
Around 250 face-to-face sessions have taken place with highly vulnerable people, leading one homeless person to become a volunteer on a regular basis.
Anchor programme
Hospitals and councils are major local employers and procurers of services. The anchor approach sees these institutions as important resources for local change. In mid and south Essex, anchor is linking these institutions with community projects.
The projects help residents develop employment skills and then support people into work, providing economic development and much-needed staffing.
Community food market
The St Vincent de Paul Society food market, delivered by Southend City Council with the Food Alliance, arranges fortnightly visits from a mobile food van.
The van targets deprived areas with low food provision, including sheltered accommodation sites. Customers buy £15–20 worth of food for just £3.50 and are signposted to services offering support with issues including health, social care, housing, benefits and social networks.
Our key areas of focus
Our work on health inequalities is guided by the national NHS CORE20 PLUS5 frameworks.
Definition
CORE20 refers to the most deprived 20% of the national population, as identified by the national Index of Multiple Deprivation.
A snapshot of deprivation in mid and south Essex
- 133,000 people live in the most 20% most deprived areas nationally. 10.5% of the whole population of mid and south Essex.
- Mid Essex
- 5,236 live in areas of high deprivation (1% of the population)
- South East Essex
- 58,818 live in areas of high deprivation (15% of the population)
- Basildon and Brentwood
- 48,217 live in areas of high deprivation (17% of the population)
- Thurrock
- 21,271 live in areas of high deprivation (11% of the population)
Examples of what we are doing to improve health in the CORE20
The PLUS groups
Definition
PLUS groups are population groups that may experience poorer than average health access, experience or outcomes across their communities.
Examples of work happening across MSE with the PLUS group communities
- Members of ethnic minority groups. Southend Victoria PCN is inviting BAME women to smear tests by phone rather than sending a standard letter.
- Children with neurodiversity, special educational needs and disabilities. A youth co-production project is testing accessibility of clinical services using virtual reality.
- Veterans. GPs are receiving specialist training to offer tailored veteran support.
- People experiencing homelessness – Sanctus Homeless Charity is hosting a one-stop health and wellbeing service.
- Carers. The Mid Essex Alliance is running a project to support young carers.
- Learning disability. A co-design project with Healthwatch Essex is developing service improvements.
- Gypsy, Roma and the traveller communities. A mobile clinic is delivering preventative health across sites in Basildon and Thurrock.
The patients I see who live in less affluent areas will often have come in with complex needs – not just medical needs but social needs such as substance misuse issues, poor housing and smoking-related conditions. They may also need translators or have other access needs. A GP can’t tackle all that in one short appointment. This is why we need a strategic approach.
Dr Kristina Rusakoviene MRC GP, Queensway Surgery | Respiratory Lead and Health Inequalities lead, Southend Victoria PCN | National Trailblazer Deprivation Fellow
Five clinical priorities
The CORE20 PLUS5 frameworks set out five clinical priorities for adults (maternity, serious mental illness, respiratory, cancer and hypertension) and five for children and young people (asthma, diabetes, epilepsy, oral health and mental health)
Examples of work happening across MSE on the clinical priorities
- People with severe mental illness. As part of the NHS Innovation Accelerator programme, MSE is improving uptake of health checks, including home visits for people with the greatest need.
- Maternity. We launched a new smoke-free pathway, with hospitals providing smoking cessation support and tobacco replacement options
- Early cancer diagnosis. A programme being rolled out across MSE has screened more than 17,000 local people, resulting in treatment for more than 100 people with previously undiscovered lung cancer
- Hypertension. More than 92,000 residents took part in a monitoring programme, with GPs in deprived areas receiving 2,000 extra blood pressure machines
- Mental health in children and young people. We recruited 13 PCN-based mental health practitioners specialising in children and young people, to support access to services
- Asthma in children and young people. We promoted a tool to help children and families learn more about asthma, triggers and effective management
Health inequalities funding
The MSE ICB has committed £3.4 million each year to reduce health inequalities.
In each alliance, we’re working through trusted partners – either community and voluntary sector infrastructure organisations or local councils – to identify and support projects that narrow the gap in health inequalities.
Our funding is focused on the most deprived communities, PLUS groups, clinical priority areas or priority lifestyle behaviours such as smoking and weight management. The aim is to test new, innovative and collaborative approaches to addressing the underlying causes of health inequalities.
The University of Essex is helping evaluate the schemes so we can learn what works and how to scale and spread these approaches across the populations most at need.
Where our funding goes
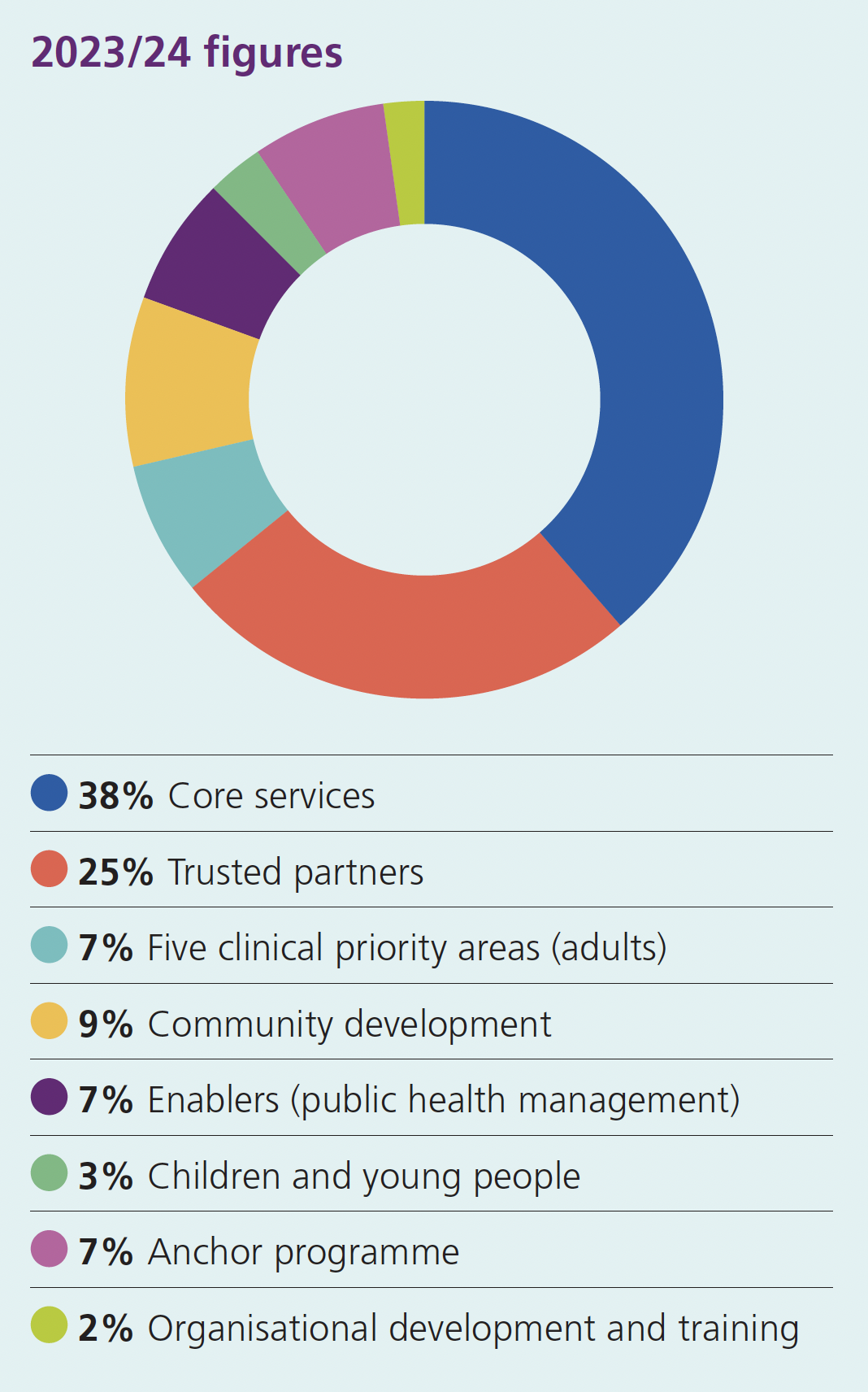
Where our funding goes
The image is a pie chart illustrating the allocation of funding for the year 2023/24. The chart is divided into different coloured segments, each representing a specific area of funding. Here is a plain text description of the information presented:
Core services: 38% (blue)
Trusted partners: 25% (red)
Five clinical priority areas (adults): 7% (teal)
Community development: 9% (yellow)
Enablers (public health management): 7% (purple)
Children and young people: 3% (green)
Anchor programme: 7% (magenta)
Organisational development and training: 2% (light green)
- Core services – £1,307,654
- Trusted partners – £854,062
- Five clinical priority areas (adults) – £238,940
- Community development – £322,914
- Enablers (public health management) – £245,000
- Children and young people – £100,000
- Anchor programme – £250,000
- Organisational development and training – £81,430
Working towards shared goals
Tackling health inequalities is a joint effort between the people at every level, across multiple sectors. We asked four people in the system to share how they see their role in achieving our shared ambition.
Voluntary organisation:
We listen to local people’s experiences of using health and care services. We share key messages with partners and support and challenge partners to make sure residents’ voices are heard. Triangulating hard data with lived experience is critical, giving insight into the challenges faced by local people wanting to lead healthier lives.
Owen Richards, Chief Officer, Healthwatch Southend
Provider:
We are the only acute provider within the ICB with local communities accessing our services across the geography. Improving equity has been one of our key strategic goals since 2021, and since then we have collaborated with the ICB to improve communities’ access, outcomes and experience, through initiatives like anchor and our Better Letters programme.
Preeti Sud, Director of Strategy and Innovation, Mid and South Essex NHS Foundation Trust
Alliance:
The Thurrock Alliance Better Care Together Strategy offers the health sector the opportunity to work with other ICS stakeholders, including local authorities, the voluntary sector and local communities. Together, we are creating opportunities for everyone to access quality care, stable jobs, a thriving environment, and good housing and education.
Aleksandra Mecan, Director, Thurrock Alliance
System:
Developing our strategic approach to inequalities improvement is the key step to embedding an equity mindset and coordinating our efforts. By identifying the principal drivers of poorer outcomes, we can prioritise and focus on impactful actions on multiple levels to address health and wider social needs.
Dr Sophia Morris, System Clinical Lead for Inequalities, Mid and South Essex Integrated Care System
Get involved
This impact report highlights a wealth of activities taking place across mid and south Essex to narrow the health inequality gap.
But this is just the beginning.
We’ve seen that health inequalities are preventable – but to make real progress we need to build momentum. That means everyone across the health and care system pausing to consider what difference they can make.
What can you do?
Incorporating health inequalities is not always about doing more. Often, it’s about taking a fresh look at what we’re already doing and examining it from different perspectives. Start with these steps:
- Start with the data. Understand where the health inequalities are where you work. Talk to partners to see if your insights tally with theirs. Find out if there’s already work going on that you can build on.
- Engage with communities and other partners working in the field. Find out what they are experiencing, what’s already in place and what they need.
- Devise an intervention. Collaborate with those partners and ask for feedback.
- Plan how you will measure your impact. How will you know if it is working?
- Have a go! Using small cycles of change (Plan, Do, Study, Act) enablers you to start small and continuously check and adjust.
- Stay connected. Tell us what has worked well and how things could be improved so that we can learn together and create a movement to narrow the gap in health inequalities.
Using an anchor approach
We, and many of our partners, use our position as anchor institutions to overcome health inequalities through our roles as major employers and commissioners of services. There are many opportunities to boost local economies. Find out more.